Introduction One of the most common questions that practitioners ask us is what the best lens or strategy is to control myopia in children. Most of them do not practice orthokeratology and are looking for a single method that could be effective and user-friendly, both for patients and for themselves.
The first consideration is that there is no one-size-fits-all treatment approach that will work for everyone. Each child is different and should be treated in a personalized way. The analysis of one patient will be different from that of the next even if they are the same age, the same sex, the same ethnicity and are presenting similar clinical data, they do not have the same physiological basis and long-term risk factors.
It is in this perspective that we are interested in analyzing three commercial lenses used for the control of myopia, some off-label. Are they equally effective, or is there one that should be favored over the others? And under what circumstances? To answer these questions, there are two possible approaches. The first, classic, approach is to adapt groups of patients with one or the other of these lenses, in a randomly determined order, and to compare their evolution over 2 years with a control group equipped with glasses. This approach is scientifically rigorous but costs a lot of money and represents a heavy investment in time. We do not have quick answers, and if this approach is not conclusive, it is necessary to repeat the tests over a longer period of time with other products. We will never live long enough to do it all.
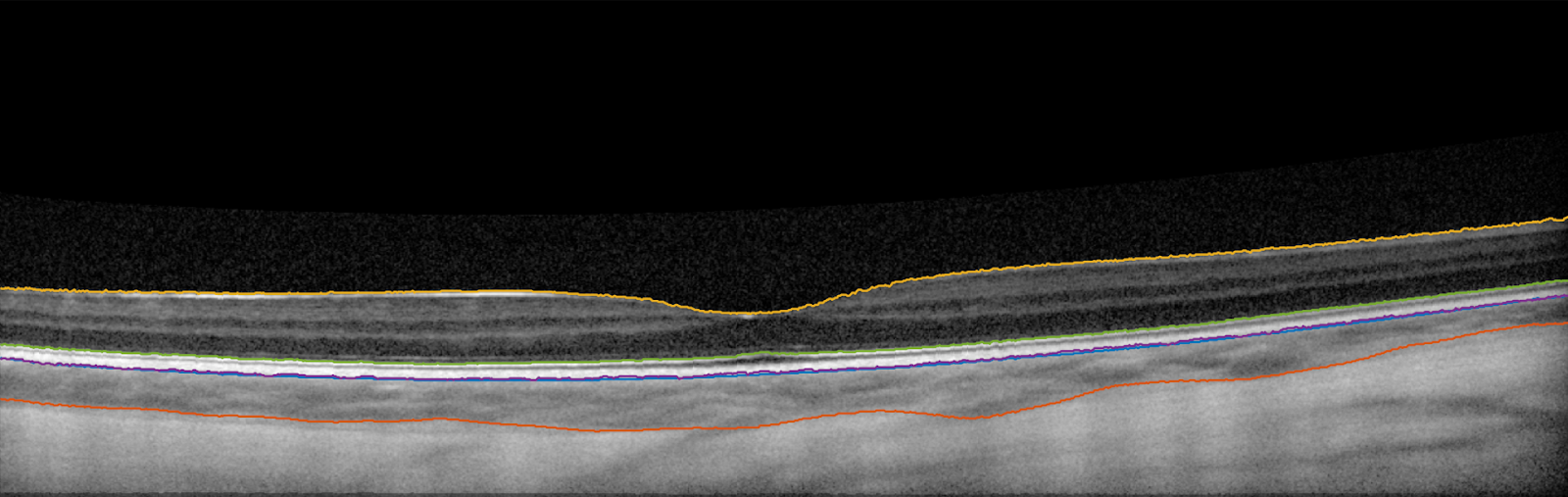
Another more pragmatic approach makes it possible to carry out short-term experiments to determine which are the most relevant elements to subsequently conduct a longitudinal study. This can save time and money while testing multiple hypotheses, without spending decades to find answers to our questions. This method is based on analyzing the variation of the choroid in response to optical stimuli. Indeed, in recent years, studies have shown that the short-term choroidal response can be considered as a valid indicator of the effectiveness of an optical device used in the management of myopia. Although there is no consensus on the technical parameters, it is agreed that a measurement with an optical coherence tomographer (OCT) allowing acquisition of quality images of the choroid is a must. Determining the choroidal thickness is then done manually or via image analysis with a given software. The use of artificial intelligence has a specific niche here. In general, when the visual stimulus involves thickening of the choroid, it is agreed that this response is considered positive and therefore promotes better control of the elongation of the eye. Conversely, when the visual stimulus leads to thinning of the choroid, it is agreed that this signal encourages the progression of myopia and axial length.
METHODS & LENSES TESTED
We recruited a cohort of 24 Caucasian young adults (12 F/12M 25.8 ± 3.5 y.o.) who had moderate myopia (-2.58D ± 1.48D). All had best-corrected visual acuity (BCVA) of 20/20 or better monocularly and binocularly, and none had been diagnosed with ocular pathology. Participants were asked to not wear contact lenses for 72 hours prior to testing. Activities and nutrition were controlled 24 hours before and on the day of the testing (refraining from athletic training or strenuous exercises, stimulating food, caffeine, alcohol, tobacco, etc.).
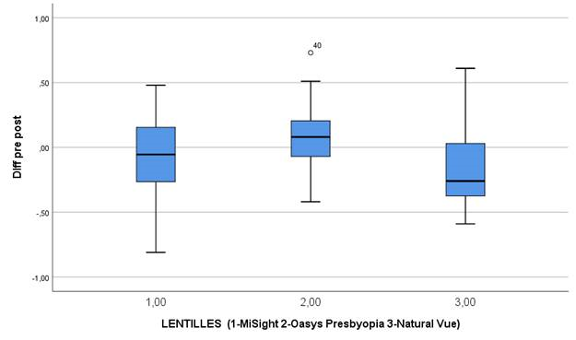
Three different soft multifocal contact lenses were selected: senofilcon A (Acuvue Oasys for Presbyopia, J&J Vision Care) omafilcon A (MiSight, CooperVision) and etafilcon A (NaturalVue, Visioneering Technology). Lenses were randomly fitted on every participant. The lenses were worn for 30 minutes followed by a 20-minute washout period. Throughout the experiment, participants had to read a book without images or watch a (boring) film that did not generate strong emotions or display much action.
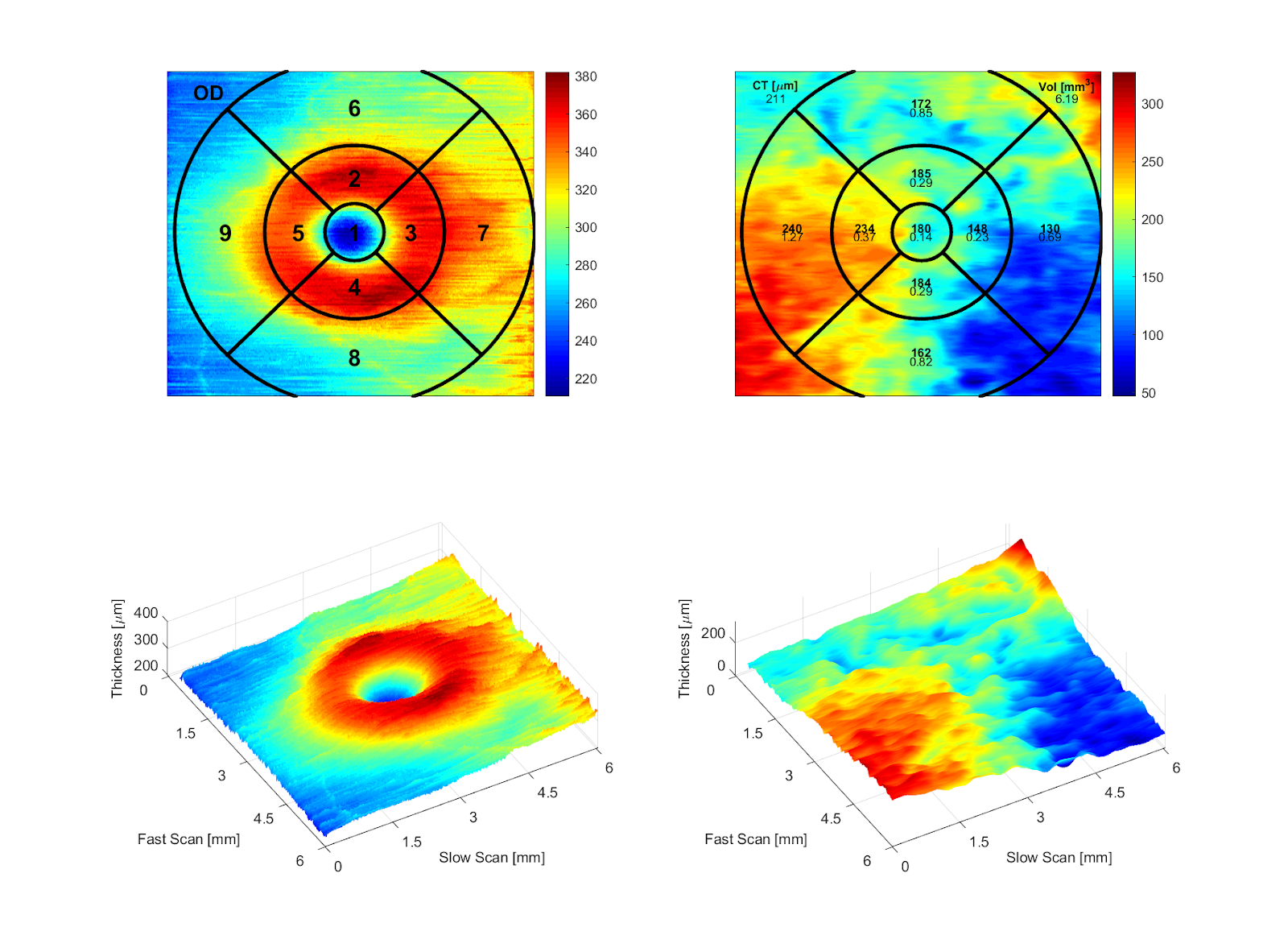
Images were taken with a confocal scanning laser ophthalmoscope (cSLO, Heidelberg Spectralis) featuring an active eye tracking and AutoRescan software, which ensures that the measured variations were based on the same locations on the retina, corresponding to the previous measurements at 100%. Images were then processed through a proprietary matlab software that was able to evaluate not only the thickness of the choroidal tissue but also its volume [1], which is more important and clinically relevant. Detection of the choroidal margins was automated with the use of artificial-intelligence-based software, following the ETDRS approach by quadrant [2].